Rotator Cuff Injuries
Rotator Cuff Injuries
We’ve all heard of our rotator cuff, but what role does it play in our everyday movement and how does an injury affect us?
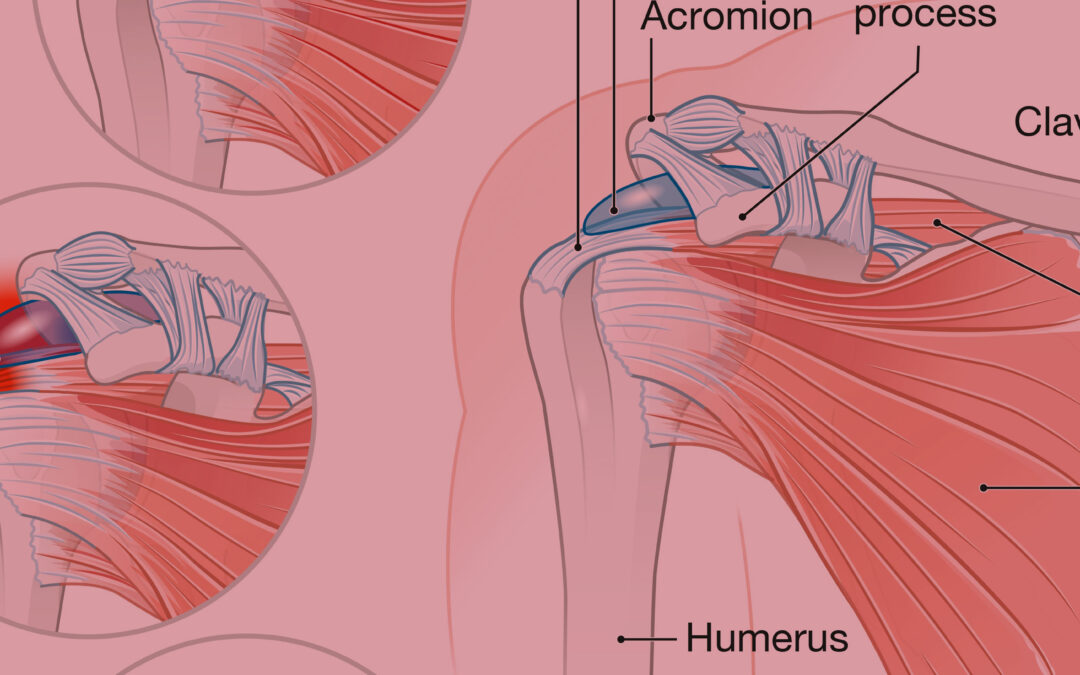
The rotator cuff plays a crucial role in moving and stabilizing the shoulder, allowing for a wide range of movements. It is vital for maintaining shoulder stability and enabling proper shoulder function. It helps keep the upper arm bone dynamically centred within the shoulder socket, allowing for smooth and coordinated movements. So, how do we injure it?
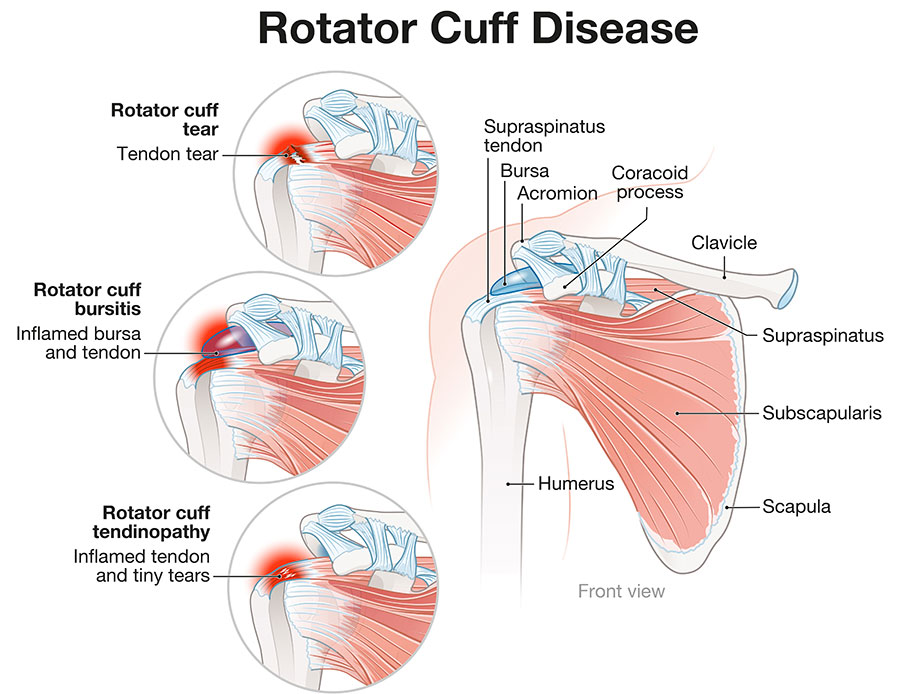
A rotator cuff injury refers to damage or tears in the group of muscles and tendons that surround the shoulder joint. Common causes of rotator cuff injuries include repetitive overhead motions, trauma or injury, and age-related degeneration. Whether it’s due to a sudden injury or gradual wear and tear, a rotator cuff injury can significantly impact a person’s quality of life, limiting their ability to perform tasks such as lifting, reaching, or throwing. It is often painful and can lead to weakness, limited range of motion, and difficulty performing everyday activities.
It is important to promptly seek appropriate treatment to alleviate pain, restore strength, and improve overall shoulder function.
Physiotherapy is an effective treatment option for rotator cuff injuries. A physiotherapist will evaluate the severity of the injury, assess the range of motion and strength of the shoulder, and develop a customized treatment plan.
Initially, treatment may focus on reducing pain and inflammation through techniques like ice therapy, electrotherapeutic modalities, and gentle exercises. As the healing progresses, physiotherapy will involve a combination of strengthening exercises to target the muscles of the rotator cuff, as well as stretches to improve flexibility. Manual therapy techniques such as joint mobilization and soft tissue massage may also be employed to enhance shoulder mobility and reduce muscle tension.
Through a progressive rehabilitation program, physiotherapy aims to restore strength, stability, and function to the shoulder, enabling individuals to regain their normal activities and prevent future injuries.
